Presurgical MRI to predict risk of chronic kidney disease: AuntMinnie Article Summary
Purpose: Patients with solid renal masses (SRMs) are at risk of chronic kidney disease (CKD) after surgical resection with- out a reliable pre-operative predictor. This study investigates whether pre-operative multiparametric MRI (mpMRI) can predict CKD development and progression to stage 3 CKD.
Methods: 43 patients at the Icahn School of Medicine scheduled to undergo partial or radical nephrectomy for a localized solid renal mass agreed to a presurgical MRI including T1, R2*, ASL, and 9-bvalue DWI. We also obtained histopathological tumor characterization, and measures of kidney function at baseline and at 12months after surgery with serum creatinine estimated glomerular filtration rate (eGFR). We also calculated a clinical CKD risk score from eGFR, age, diabetes status, and surgery technique following the simplified calculation proposed by Ellis et al. (2020): +1 point for age>65years, +1 point for history of diabetes, +3 points for radical nephrectomy, and +3 for eGFR < 90 mL/min/1.73 m2, with an added +1 if eGFR < 80, and another added +1 if eGFR < 70. It’s proposed that a higher clinical CKD risk score = higher risk of CKD after surgery.
Results: Thirty of 43 (67%) participants had normal baseline renal function (eGFR>60mL/min/1.73m2). Of the 29 participants who completed 12-month follow-up, 66% (19/29) had baseline normal eGFR with 37% (7/19) developed stage 3 CKD. 30% had baseline stage 3 CKD and 48% had an eGFR decline > 5 mL/min/1.73m2.
eGFR from DCE-MRI and tubule diffusion correlated with baseline eGFR (r2 = 0.43 and 0.33 respectively). Reduced vascular diffusion from multi-b-value DWI MRI predicted eGFR decline (AUC=0.75–0.83, DOR=6.8–16.5), and lower vascular diffusion also correlated with a greater amount of decline after surgery. The clinical risk score was not predictive of renal decline. A higher CKD clinical risk score was associated with CKD development and showed acceptable discriminative performance (AUC = 0.81) with high specificity but low sensitivity (specificity = 0.92, sensitivity = 0.33). A larger contralateral ADC corticomedullary difference (AUC = 0.89; DOR = 22.5) had the highest predictive ability with high sensitivity (0.83) and specificity (0.82).
Conclusions: Pre-operative mpMRI may provide complementary information to clinical measures for predicting CKD progression and functional deterioration post-nephrectomy and allows assessment of individual kidney function in patients undergoing surgical management of renal masses. While pre-surgical MRI is commonly acquired to characterize renal masses, the coinciding information of the renal parenchyma can provide biologically specific biomarkers of renal pathology and physiology. As kidney-protective therapies emerge, and management options include active surveillance and focal ablation, identifying high-risk patients before surgery is critical to guide decision-making, personalize treatment, and prevent end-stage kidney disease.
Integrating imaging biomarkers with clinical and laboratory data to capture overall patient health and organ-specific health could yield a robust, precise and sensitive personalized predictor of CKD risk.
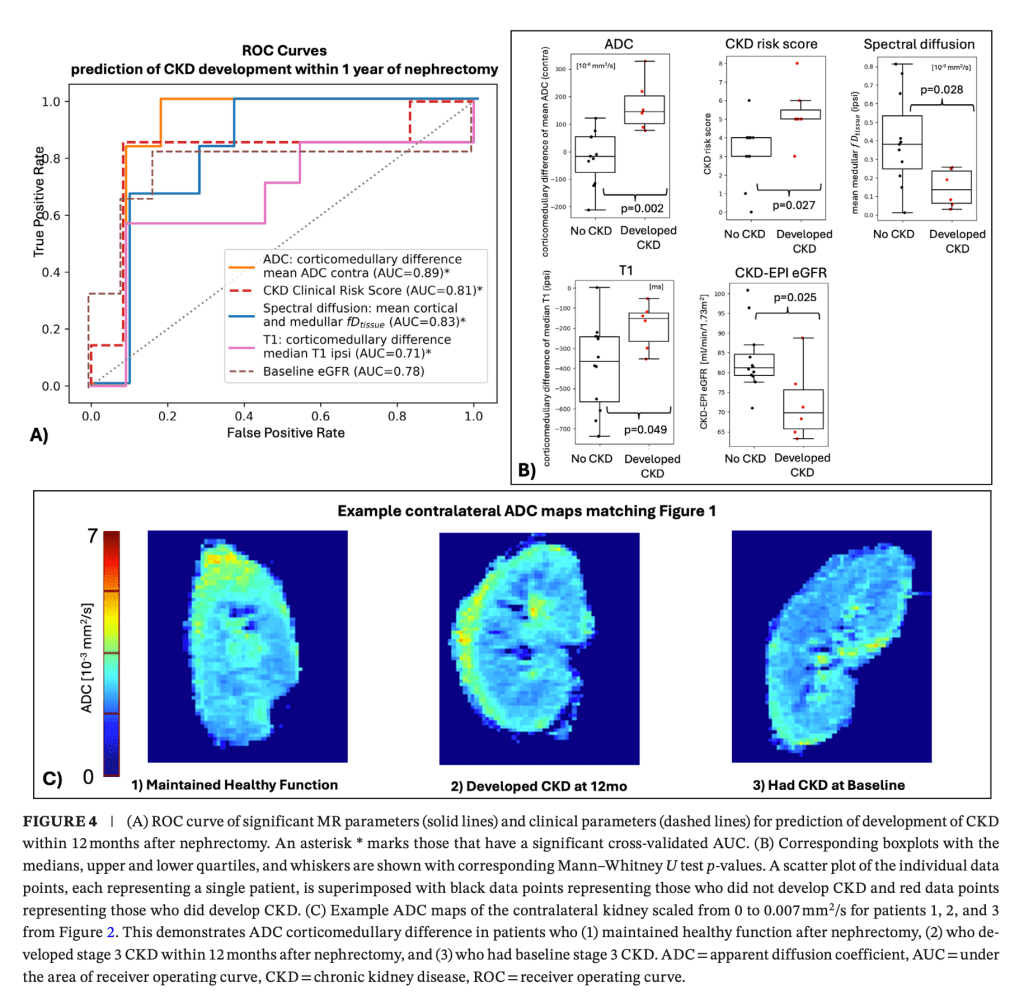
Figure from Multiparametric MRI for Predicting Renal Function Deterioration and Chronic Kidney Disease Development in Patients Undergoing Nephrectomy for Renal Masses: A Pilot Study, Journal of Magnetic Resonance Imaging (2026)
List of some publications relevant to this topic:
M. Liu, O. Bane, X. Mu. et al. Multiparametric MRI for Predicting Renal Function Deterioration and Chronic Kidney Disease Development in Patients Undergoing Nephrectomy for Renal Masses: A Pilot Study, 2025. DOI: 10.1002/jmri.70213
R. J. Ellis, S. J. Del Vecchio, K. M. J. Gallagher, et al., “A Simple Clin- ical Tool for Stratifying Risk of Clinically Significant CKD After Ne- phrectomy: Development and Multinational Validation,” Journal of the American Society of Nephrology (2020). DOI: 10.1681/asn.2019121328.
R. J. Ellis, “Chronic Kidney Disease After Nephrectomy: A Clinically- Significant Entity?,” Translational Andrology and Urology (2019). DOI: 10.21037/tau.2018.10.13.
S.-H. S. Huang, A. P. Sharma, A. Yasin, R. M. Lindsay, W. F. Clark, and G. Filler, “Hyperfiltration Affects Accuracy of Creatinine eGFR Measurement,” Clinical Journal of the American Society of Nephrology (2011). DOI: 10.2215/cjn.02760310.
D. Chae, N. Y. Kim, K. J. Kim, K. Park, C. Oh, and S. Y. Kim, “Pre- dictive Models for Chronic Kidney Disease After Radical or Partial Nephrectomy in Renal Cell Cancer Using Early Postoperative Serum Creatinine Levels,” Journal of Translational Medicine (2021). DOI: 10.1186/s12967-021-02976-2.
L. Berchtold, L. A. Crowe, C. Combescure, et al., “Diffusion- Magnetic Resonance Imaging Predicts Decline of Kidney Function in Chronic Kidney Disease and in Patients With a Kidney Allograft,” Kidney International (2022). DOI: 10.1016/j. kint.2021.12.014.
M. Liu, O. Bane, X. Mu. et al. Immuno-Oncologic Profiling of Renal Masses using Multiparametric MRI: A Pilot Study. Journal of ImmunoTherapy of Cancer, 2025; DOI: 10.1136/jitc-2025-012833
M. Liu, T. Gladytz, J. Dyke et al. Estimation of Multi-Component Flow in the Kidney with Multi-b-value Spectral Diffusion. Magn Reson Med. 2025. 10.1002/mrm.30644
M. Liu, J. Dyke, T. Gladytz et al. Detecting early kidney allograft fibrosis with multi-b-value spectral diffusion MRI. Sci Rep. 10.1038/s41598-025-24701-5
JS Periquito, T. Gladytz, JM Millward et al. Continuous diffusion spectrum computation for diffusion-weighted magnetic resonance imaging of the kidney tubule system. Quantitative Imaging in Medicine and Surgery. 2021. 10.21037/qims-20-1360.
J. Stabinska, A. Ljimani, HJ Zöllner et al. Spectral diffusion analysis of kidney intravoxel incoherent motion MRI in healthy volunteers and patients with renal pathologies. Magnetic Resonance in Medicine. 2021. 10.1002/mrm.28631.
J. Stabinska, HJ Wittsack, LO Lerman, et al. Probing Renal Microstructure and Function with Advanced Diffusion MRI: Concepts, Applications, Challenges, and Future Directions. Journal of Magnetic Resonance Imaging. 2023;doi:10.1002/jmri.29127
EE Sigmund, PH Vivier, D Sui, et al. Intravoxel Incoherent Motion and Diffusion-Tensor Imaging in Renal Tissue under Hydration and Furosemide Flow Challenges. Radiology. 2012. 10.1148/radiol.12111327.
A. Ljimani, A. Caroli, C. Laustsen et al. Consensus-based technical recommendations for clinical translation of renal diffusion-weighted MRI. Magnetic Resonance Materials in Physics, Biology and Medicine. 2019. 10.1007/s10334-019-00790-y.
A. Caroli, M. Schneider, I. Friedli, et al. Diffusion-weighted magnetic resonance imaging to assess diffuse renal pathology: a systematic review and statement paper. Nephrology Dialysis Transplantation. 2018. doi:10.1093/ndt/gfy163
O. Bane, M. Wagner, JL Zhang, et al. Assessment of renal function using intravoxel incoherent motion diffusion‐weighted imaging and dynamic contrast‐enhanced MRI. Journal of Magnetic Resonance Imaging. 2016; doi:10.1002/jmri.25171
R. van der Bel, OJ. Gurney-Champion, M. Froeling et al. A tri-exponential model for intravoxel incoherent motion analysis of the human kidney: In silico and during pharmacological renal perfusion modulation. European Journal of Radiology. 2017. doi:10.1016/j.ejrad.2017.03.008
Federau C. Intravoxel incoherent motion MRI as a means to measure in vivo perfusion: A review of the evidence. NMR in Biomedicine. 2017; doi:10.1002/nbm.3780
AL Liu, A Mikheev, H. Rusinek H, et al. REnal Flow and Microstructure AnisotroPy (REFMAP) MRI in Normal and Peritumoral Renal Tissue. Journal of Magnetic Resonance Imaging. 2018. doi:10.1002/jmri.25940
M. Liu, O. Bane, H. Al-Mubarak, A. Reddy, P. Kennedy, P. Robson, J. Cuevas, K. Meilika, A. Horowitz, B. Kuhn, K. Badani, B. Taouli, S. Lewis. Assessment & Prediction of Renal Function with Non-Contrast MRI in Patients Undergoing Surgical Management of Solid Renal Masses.” International Society for Magnetic Resonance in Medicine Workshop on IVIM 2024. (Oral Presentation)
